
 February 8, 2026
February 8, 2026  9 Min
9 Min  No Comment
No Comment 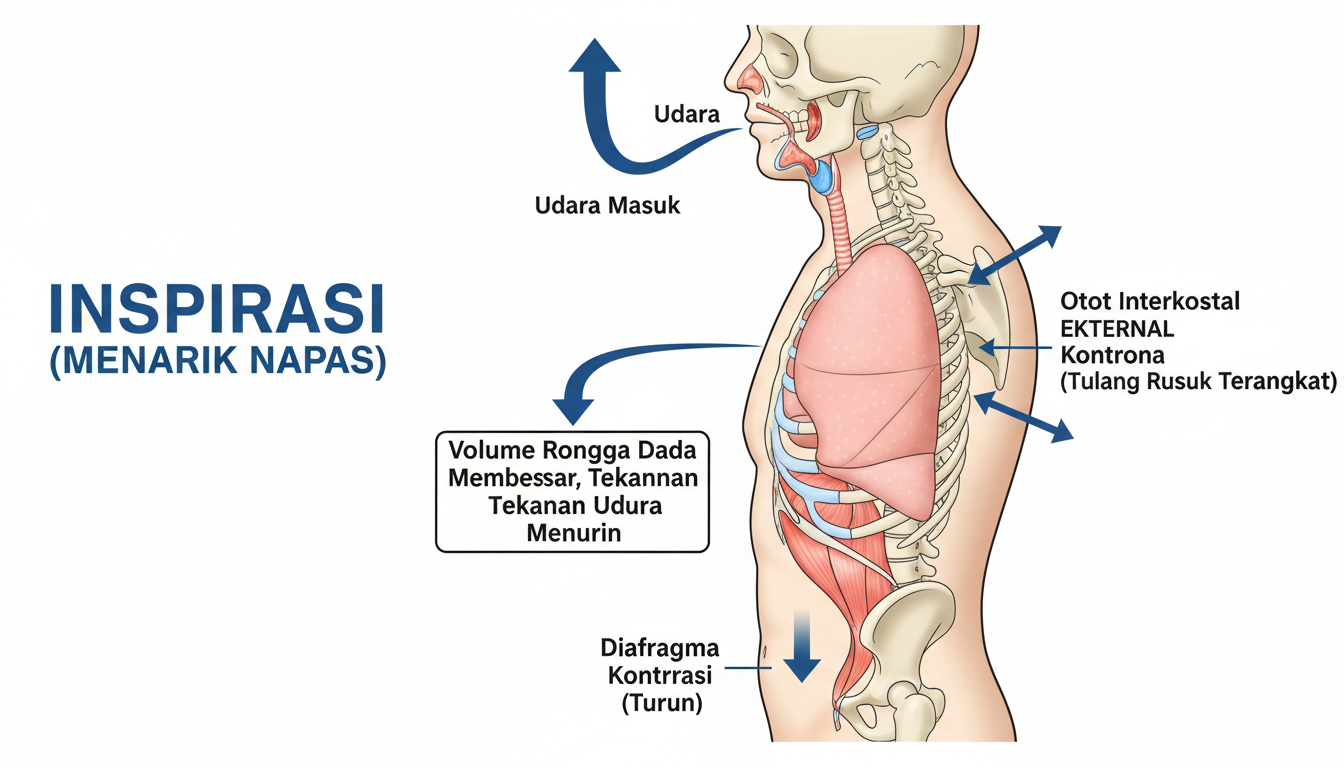
\`\`\`html
The physics of breathing unfold with every chest rise and fall—muscle contractions, pressure gradients, and neural feedback working in concert you’ve likely never considered twice. In my years studying human physiology and working with patients experiencing breathing difficulties, I’ve come to appreciate how elegantly these mechanisms adapt: climbing stairs, sleeping soundly, or preparing for a high-stakes presentation all demand different respiratory responses. Sometimes the system falters—through illness, altitude shifts, or even slouching at a desk. Let me explain what’s happening inside your chest right now.
The Big Picture: How Inspiration and Expiration Work Together
The respiratory system coordinates multiple anatomical structures—lungs, diaphragm, intercostal muscles, and airways—to move air in and out of the body. Healthy adults typically breathe 12–20 times per minute at rest, moving approximately 5–8 liters of air per minute during normal respiration. Inspiration delivers fresh oxygen to the alveoli; expiration removes carbon dioxide waste. These actions involve pressure dynamics, muscular coordination, and feedback loops that maintain body function.
Why It Matters
- Oxygen fuels cellular metabolism and ATP production—without efficient intake, energy systems falter.
- Carbon dioxide must be eliminated to maintain blood pH between 7.35–7.45, preventing respiratory acidosis.
- The respiratory system dynamically adjusts: resting breathing differs dramatically from exercise-induced hyperventilation, with minute ventilation increasing from approximately 6 L/min to over 100 L/min during intense exertion.
For readers searching “mechanism of inspiration and expiration in human respiratory system,” clarity and practical examples make the difference between confusion and understanding.
Mechanism of Inspiration (Inhalation)
Anatomical Movers and Shakers
Inspiration relies on two primary muscle groups: the diaphragm and external intercostal muscles. Visualizing the diaphragm as a dome-shaped structure helps grasp its function—when it contracts, this dome flattens and descends.
- Diaphragm contraction: Flattens downward, expanding the thoracic cavity vertically by approximately 1–2 cm during quiet breathing.
- External intercostals: Contract to elevate the rib cage, increasing chest width and anterior-posterior dimensions by roughly 5 cm.
This coordinated expansion lowers intrathoracic pressure from approximately -5 cm H₂O to about -8 cm H₂O below atmospheric pressure, creating a pressure gradient that draws air into the lungs. This follows Boyle’s Law: as volume increases, pressure decreases, and air flows from higher to lower pressure zones.
The Pressure Gradient Dance
During inspiration, intrathoracic pressure drops below atmospheric pressure, creating the pressure differential necessary for airflow. Air enters through the nasal passages or mouth, travels through the pharynx and larynx into the trachea, branches into main bronchi, and continues through increasingly smaller bronchioles until reaching the approximately 300 million alveoli where gas exchange occurs. The human lung contains roughly 300 million alveoli, providing a total surface area for gas exchange of approximately 70 square meters.
In clinical settings, nasal obstruction or heavy speech often triggers mouth-breathing—the same physical principles apply regardless of entry point.
Real-Life Application
Consider sprinting to catch a departing bus. The diaphragm and intercostals contract more forcefully, tidal volume can increase from approximately 500 mL to 2–3 liters per breath, and accessory muscles (scalenes, sternocleidomastoid) engage to further expand the chest wall. During maximal exercise, minute ventilation can exceed 150 L/min in healthy adults.
Mechanism of Expiration (Exhalation)
Passive vs. Active Expiration
During quiet breathing at rest, expiration is predominantly passive. The diaphragm relaxes, elastic fibers in lung tissue recoil, and the chest wall returns to its resting position. Intrathoracic pressure rises above atmospheric pressure, pushing air out without muscular effort. However, during exertion, coughing, or vocalization, expiration becomes actively controlled.
- Passive expiration:
- Diaphragm and external intercostals relax.
- Elastic recoil of lungs and chest wall reduces thoracic volume.
- Air exits passively due to pressure differentials.
-
Active expiration:
- Internal intercostals contract, depressing the rib cage.
- Abdominal muscles (external oblique, internal oblique, transversus abdominis, rectus abdominis) compress abdominal contents, pushing the diaphragm upward.
- Intrathoracic pressure can exceed atmospheric pressure by 30–50 cm H₂O during forceful expiration, enabling rapid airflow.
In my work with singers and public speakers, controlled active expiration proves essential for voice projection and modulation.
Pressure Dynamics During Expiration
Active expiration generates positive intrathoracic pressure that serves multiple functions: expelling air rapidly, clearing airways through coughing, and assisting in intra-abdominal pressure regulation for core stability. Lung compliance—the relationship between lung volume and pressure—determines how easily this occurs; high compliance (as in emphysema) makes expiration more difficult.
Real-World Scenario
When someone delivers a public speech, expiration must be precisely controlled. The speaker modulates airflow through the glottis to produce consistent volume and pitch, requiring coordinated abdominal contraction and glottal adjustment—active expiration balancing pressure dynamics with vocal needs.
Integrated Respiratory Cycle at Work
Continuous Transition
A complete respiratory cycle involves smooth transitions between phases:
- Diaphragm contracts → thoracic volume increases → intrathoracic pressure drops below atmospheric → air enters lungs.
- Diaphragm relaxes → thoracic volume decreases → intrathoracic pressure exceeds atmospheric → air exits lungs.
Real-world breathing rarely follows this idealized pattern. Stress can accelerate respiratory rate to 25–30 breaths per minute, anxiety often produces shallow breathing, and various pathologies disrupt normal mechanics.
Control Mechanisms
- Chemoreceptors in the medulla and carotid bodies detect PaCO₂ changes as small as 2–3 mmHg, adjusting ventilation accordingly.
- Central command allows voluntary overrides—holding breath or deliberately hyperventilating.
- Protective reflexes like coughing (triggered by irritant receptors) and sneezes modify expiration to clear airways.
The system integrates automatic regulation with conscious control—a sophisticated balance between involuntary stability and voluntary flexibility.
Clinical Considerations: When Mechanics Disrupt
Conditions Affecting Respiratory Mechanics
- Asthma: Bronchoconstriction increases airway resistance, prolonging expiration and trapping air; patients compensate with increased respiratory rate (often exceeding 20 breaths/minute). Airway resistance during severe bronchoconstriction can increase 5–10 fold.
- COPD: Destruction of elastic tissue reduces recoil pressure, while airway collapse during expiration causes air trapping; dynamic hyperinflation can reduce effective ventilation significantly. Emphysema destroys approximately 50% of alveolar walls in severe cases.
- Pleural effusion: Fluid accumulation (can exceed 2 liters in large effusions) restricts lung expansion and reduces tidal volume.
- Pneumothorax: Air in the pleural space eliminates negative pressure, causing lung collapse.
- Neuromuscular disorders: Weakness of respiratory muscles impairs both phases; diaphragmatic strength can decline substantially in conditions affecting motor neurons. When vital capacity falls below 50% predicted, mechanical ventilation may become necessary.
Clinicians assess these conditions using spirometry (measuring FEV1, FVC, and their ratio), body plethysmography for lung volumes, and arterial blood gas analysis to evaluate gas exchange efficiency.
Therapeutic Interventions
- Bronchodilators (beta-2 agonists, anticholinergics) reduce airway smooth muscle tone, decreasing resistance during expiration.
- Positive pressure ventilation (CPAP, BiPAP) maintains airway patency and assists muscle function.
- Pulmonary rehabilitation strengthens respiratory muscles and optimizes breathing patterns.
These approaches underscore the delicate balance required for effective respiration.
Cross-System Interactions
Cardiovascular Connection
Breathing directly affects cardiac function. During inspiration, reduced intrathoracic pressure increases venous return to the right atrium, while left ventricular output transiently decreases—the phenomenon behind respiratory sinus arrhythmia. Research examining heart rate variability responses to breathing frequencies demonstrates that slow breathing practices can enhance parasympathetic markers.
Neural Control Centers
The medullary respiratory center generates automatic rhythm, while the pons modulates inspiration duration and prevents overinflation. During stress, the hypothalamus and limbic system influence respiratory rate and depth, explaining why anxiety produces rapid, shallow breathing.
Metabolic Demands
Exercise increases oxygen consumption substantially and CO₂ production proportionally. The respiratory system responds by increasing tidal volume and respiratory rate, raising minute ventilation dramatically to meet metabolic demands.
Beyond Theory: Practical Applications
For Athletes and Performers
In my work with endurance athletes, understanding respiratory mechanics has proven essential for optimizing performance. Controlled breathing during high-intensity intervals maintains alveolar ventilation efficiency, while specific expiratory techniques support core stability during power movements. Singers benefit particularly from diaphragmatic breathing training, which allows sustained expiratory control for phrases lasting extended periods.
Stress Management Applications
Diaphragmatic breathing activates the parasympathetic nervous system through the vagus nerve. Evidence from clinical studies indicates that slow breathing practices can reduce physiological stress markers. Understanding which muscles to engage changes not just airflow but also autonomic nervous system balance.
Patient Education Value
When explaining breathing mechanics to patients using inhalers, comprehension improves significantly. Understanding that bronchodilators relax airway smooth muscle—and that proper technique ensures medication reaches the airways—increases adherence rates. Similarly, families facing mechanical ventilation benefit from understanding that the ventilator assists muscles rather than replacing normal physiology.
Human Variability in Breathing Patterns
Breathing patterns vary considerably between individuals and within the same person across contexts. Yawns—which can last several seconds and increase lung ventilation substantially—appear to reset respiratory drive and potentially cool brain tissue. Hiccups represent involuntary diaphragmatic spasms triggered by phrenic nerve irritation, demonstrating the sensitivity of respiratory control circuits.
Postural effects are substantial: slouching can reduce vital capacity notably, while upright positioning improves diaphragmatic excursion. Forward head posture and rounded shoulders restrict external intercostal function, potentially reducing tidal volume and increasing respiratory effort.
Conclusion
The mechanisms of inspiration and expiration represent elegant integration of muscular action, pressure gradients, structural mechanics, and neural regulation. From resting breathing to exercise-induced rates exceeding 40 breaths per minute, the system reconfigures continuously to meet metabolic demands.
Understanding these principles has practical value across contexts: optimizing athletic performance, managing chronic respiratory conditions, reducing stress through controlled breathing, or simply appreciating the remarkable systems operating continuously within us. The human respiratory system adapts remarkably well—a living system refined through millions of years of evolution.
FAQs
What exactly happens during inspiration at the muscle level?
Inspiration involves diaphragm contraction (flattening the dome by 1–2 cm) and external intercostal activation (elevating ribs), both increasing thoracic cavity volume, lowering intrathoracic pressure below atmospheric pressure, and drawing air into the lungs.
Why is expiration passive most of the time?
At rest, lung recoil rather than active muscle contraction achieves much of the expiratory phase. The lungs contain elastin and collagen fibers that return them to resting position after inspiration, making muscle contraction unnecessary for normal exhalation.
How does active expiration differ under stress or exertion?
During exertion, abdominal muscles and internal intercostals contract forcefully, generating intrathoracic pressures substantially higher than passive expiration. This enables rapid air expulsion for coughing, voice projection, and meeting increased metabolic demands.
How do conditions like asthma or COPD affect breathing mechanics?
Asthma increases airway resistance during expiration through bronchoconstriction, causing air trapping and prolonging expiratory time. COPD reduces elastic recoil and causes dynamic airway collapse, leading to hyperinflation that can decrease effective tidal volume significantly.
Can breathing techniques really influence other body systems?
Slow breathing activates baroreceptor reflexes and vagal pathways, influencing heart rate variability and sympathetic tone. Mindful breathing practices have demonstrated effects on stress indicators and physiological relaxation responses.
Why does posture matter for effective breathing?
Upright posture allows proper diaphragmatic descent during inspiration. Forward head posture and rounded shoulders restrict external intercostal function, potentially reducing tidal volume and increasing respiratory effort.
After exploring these mechanisms, quirks, and applications, breathing exemplifies how physical principles combine with complex biological regulation to sustain life. Every inhalation involves millions of coordinated events—physics and physiology working together invisibly inside us.

\`\`\`